Recommendations
- 1. We recommend that before quantifying the size of the kidneys, patients should be classified according to the Mayo Clinic classification for typical versus atypical morphology with renal imaging.
- 2.1. We recommend that a baseline assessment of renal size be undertaken in patients with ADPKD. The objective of these measurements is to determine which patients are suitable candidates to be considered for therapeutic intervention based on their risk of progression.
- 2.2. Although the gold standard for measuring TKV is MRI stereology, we recommend the use of ellipsoid TKV or US to determine TKV in routine clinical practice. We suggest that MRI or CT htTKV is currently the most accurate method of assessing renal size in patients with ADPKD.
- 2.3. In the absence of MRI, imaging by CT may be used to determine TKV. In situations where an MRI or CT is not easily obtainable, we suggest US-measured KL as a suitable surrogate. US can be used to determine TKV; however, TKV obtained using US may introduce error and does not provide an advantage over KL.
- 3. We recommend that routine assessment of TKV or KL should not exceed a frequency of once yearly.
Renal Imaging
Several imaging modalities are currently available to diagnose and evaluate ADPKD, including abdominal ultrasound, computed tomography (CT), and magnetic resonance imaging (MRI). In terms of diagnosis, our nephrologist survey indicated that 92% of clinicians are using US as their diagnostic modality. US has robust performance in this setting; age-based criteria and diagnostic performance have been previously published and serve as good criteria for imagingbased diagnosis.22 MRI and high-resolution US have greater sensitivity for imaging-based diagnosis at younger ages than conventional US,23 but the availability of these tests in some centers may be limited.
For size determination, MRI appears to be the preferred imaging modality; it has greater accuracy and precision when compared with US, and although CT performs well, it requires radiation exposure.24,25 US is a more practical and more cost-effective approach; however, there are concerns that, compared with CT or MRI, US is more user-dependent and has higher variability making it difficult to obtain accurate and reproducible results.26 Emerging US techniques, including 3-dimensional and high-resolution US, have some data in the diagnosis of ADPKD,23 but these modalities are not widely available, and their performance in size determination has not been evaluated.27
In ADPKD, kidney volume can be divided into cystic and noncystic components; however, changes in overall total kidney volume (TKV) are less variable than changes in either of these components individually, and TKV is easier to obtain.28 For these reasons, TKV is the more commonly used measure, and in most cases, it is unnecessary to divide the volume into cystic and noncystic components.
TKV is typically obtained either by stereology or various formulae that estimate volume from a more limited set of measurements.28,29 Stereology can be quite labor-intensive but is presently considered the gold standard for the measurement of TKV.28 The most common method of estimation is the ellipsoid equation, which has been shown to approximate the stereological approach accurately and is less laborintensive.29 Another estimation formula based on a single midcoronal measurement has also been shown to yield volumes that are highly correlated with stereology measures.30 More recently, automated methods of TKV determination have been reported to yield results similar to stereology; for these measures, patients are classified based on heightadjusted (ht) TKV and age.31,32
The nephrologist survey indicated that US is the first imaging modality in the majority of cases; the information extracted from these already available US images should be maximized, but it is important to consider the performance of this test. When measuring TKV, US tends to be more variable than MRI and tends to overestimate volume. Therefore, it may be useful to group patients into broad categories of kidney size.26 Of the component measurements, US kidney length has less variability than the other dimensions.26 US kidney length was recently found to correlate well with htTKV measured by MRI and seemed to predict the development of stage 3 chronic kidney disease (CKD) in a similar manner.33
Before interpreting TKV measurements, patients should be categorized according to the recently published Mayo Clinic Classification (Figure 1)29 (http://www.mayo.edu/research/documents/pkd-center-adpkd-classification/doc-20094754). According to this system, patients with typical symmetric, bilateral, diffuse cyst distribution are categorized as class 1 (approximately 90% of patients), whereas patients with atypical, asymmetric, or segmental cyst distribution are categorized as class 2 (Table 3). Class 1 patients can be further divided into subclasses A through E by integrating htTKV with age. Classes 1C, 1D, and 1E show the highest propensity for developing early-onset renal disease. There are subtypes of class 2 (atypical) enlargement, and class 2 patients are generally not thought to be at risk of rapid renal progression, although the original studies had too few class 2 patients to definitively comment on renal progression in this group.29
There are limited data on the role of repeated imaging.24,34 In patients where serial measurements are taken, an increase of >5% per year in TKV, corresponding to the threshold for class 1D, appears to correlate well with predicting rapid renal progression.29 Recent recommendations by the European Renal Association-European Dialysis and Transplant Association (ERA-EDTA) and the Japanese regulatory authorities also proposed that patients with an increase in TKV of >5% annually should be placed in a higher risk category for renal disease progression.35,36 If repeated measurements are obtained by the clinician, the performance of these tests should be considered. With MRI, differences in TKV can be detected with as little as a 6-month interval between measurements.37 Conversely, although US can detect differences in kidney size over many years, it is not suitable for short-term follow-up as the inherent inaccuracy in US measurements is approximately the same as the annual rate of growth.38
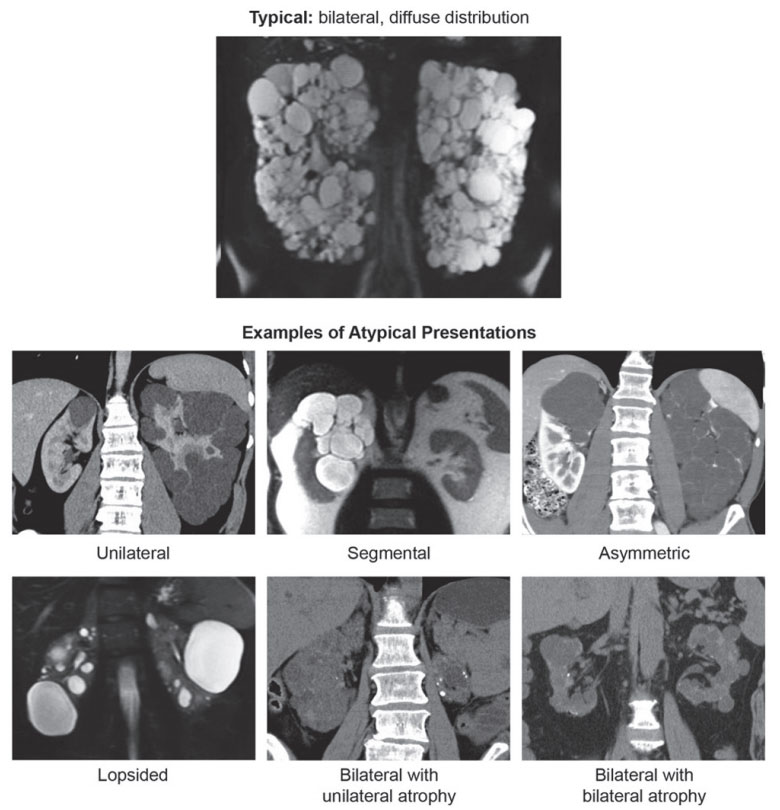
Figure 1. Mayo clinic classification of autosomal dominant polycystic kidney disease.
Source. Republished from Irazabal et al29 with permission of the American Society of Nephrology; permission conveyed through Copyright Clearance Center, Inc.
Table 3. Classification of ADPKD Based on Imaging Characteristics According to the Mayo Clinic Classification.
| Class, subclass, and term | Description |
|---|---|
| 1. Typical ADPKD | Bilateral and diffuse distribution, with mild, moderate, or severe replacement of kidney tissue by cysts, where all cysts contribute similarly to TKV |
| 2. Atypical ADPKD | |
| Unilateral | Diffuse cystic involvement of one kidney causing marked renal enlargement with a normal contralateral kidney, defined by a normal kidney volume (<275 mL in men; <244 mL in women) and having 0-2 cysts |
| Segmental | Cystic disease involving only one pole of one or both kidneys and sparing the remaining renal tissue |
| Asymmetric | Diffuse cystic involvement of one kidney causing marked renal enlargement with mild segmental or minimal diffuse involvement of the contralateral kidney, defined by a small number of cysts (>2 but <10) and volume accounting for <30% of TKV |
| Lopsided | Bilateral distribution of renal cysts with mild replacement of kidney tissue with atypical cysts where ≤5 cysts account for ≥50% TKV (the largest cyst diameter is used to estimate individual cyst volume) |
| Bilateral presentation with acquired unilateral atrophy | Diffuse cystic involvement of one kidney causing moderate to severe renal enlargement with contralateral acquired atrophy |
| Bilateral presentation with bilateral kidney atrophy | Impaired renal function (serum creatinine ≥1.5 mg/dL) without significant enlargement of the kidneys, defined by an average length <14.5 cm, and replacement of kidney tissue by cysts with atrophy of the parenchyma |
Source. Republished from Irazabal et al29 with permission of the American Society of Nephrology; permission conveyed through Copyright Clearance Center, Inc.
Note. ADPKD = autosomal dominant polycystic kidney disease; TKV = total kidney volume.