Recommendations
- We recommend that in current clinical practice, patients with a TKV measurement be categorized in terms of their risk of progression as per the Mayo Clinic classification or other validated clinical tools. We highlight that the application of the Mayo Classification to clinical practice has not yet been delineated; however, it appears to be the most robust clinical prediction tool as it pertains to the important marker of htTKV.
- Currently available TKV-based prognostication tools should not be applied to class 2 (atypical morphology)patients, as we suggest that these patients are unlikely to be rapid progressors. Certain patients may require further clinical evaluation.
- We suggest that patients who are classified as Mayo class 1C, D, or E be considered to be at risk of rapid progression of their ADPKD renal disease.
- We recommend that patients who demonstrate a sequential increase of >5% annually in TKV on imaging should be considered at risk of rapid progression of their ADPKD-related renal disease.
- We recommend that patients with an US KL of >16.5 cm bilaterally should be considered at high risk of progression of their ADPKD-related renal disease. A KL >16.5 cm has been shown to correlate with a TKV of 750 mL; however, direct measurement of TKV would be required if more accurate assessment is needed.
- We suggest that baseline TKV and KL are important determinants of renal progression of ADPKD; however, serial TKV and KL measurements have not been established as markers to monitor response to therapy.
Predicting Disease Progression
Prognostic factors related to disease progression in ADPKD include TKV, the type of genetic mutation, vasopressin activity, uric acid, and the presence of certain urine biomarkers, as summarized in Table 4.39 Disease progression in ADPKD is characterized by loss of renal function, defined as a decline of ≥5 mL/min/1.73 m2 in 1 year, or average decline of ≥2.5 mL/ min/1.73 m2 over 5 years, measured by creatinine clearance using the Cockcroft-Gault equation or by estimated glomerular filtration rate (eGFR) using the CKD-EPI equation.29,40 However, in the early stages of disease, there is little change in renal function yet detectable changes in TKV. As such, TKV is a more sensitive measure of disease progression.28
Table 4. Prognostic Factors Related to Disease Progression in ADPKD.
|
Imaging-based prognostic factors
|
|
Genetic prognostic factors
|
|
Urinary biomarkers
|
|
Other prognostic factors
|
Note. ADPKD = autosomal dominant polycystic kidney disease; TKV = total kidney volume; GFR = glomerular filtration rate; ESRD = end-stage renal disease; CRISP = Consortium of Renal Imaging Studies in Polycystic Kidney Disease; BP = blood pressure.
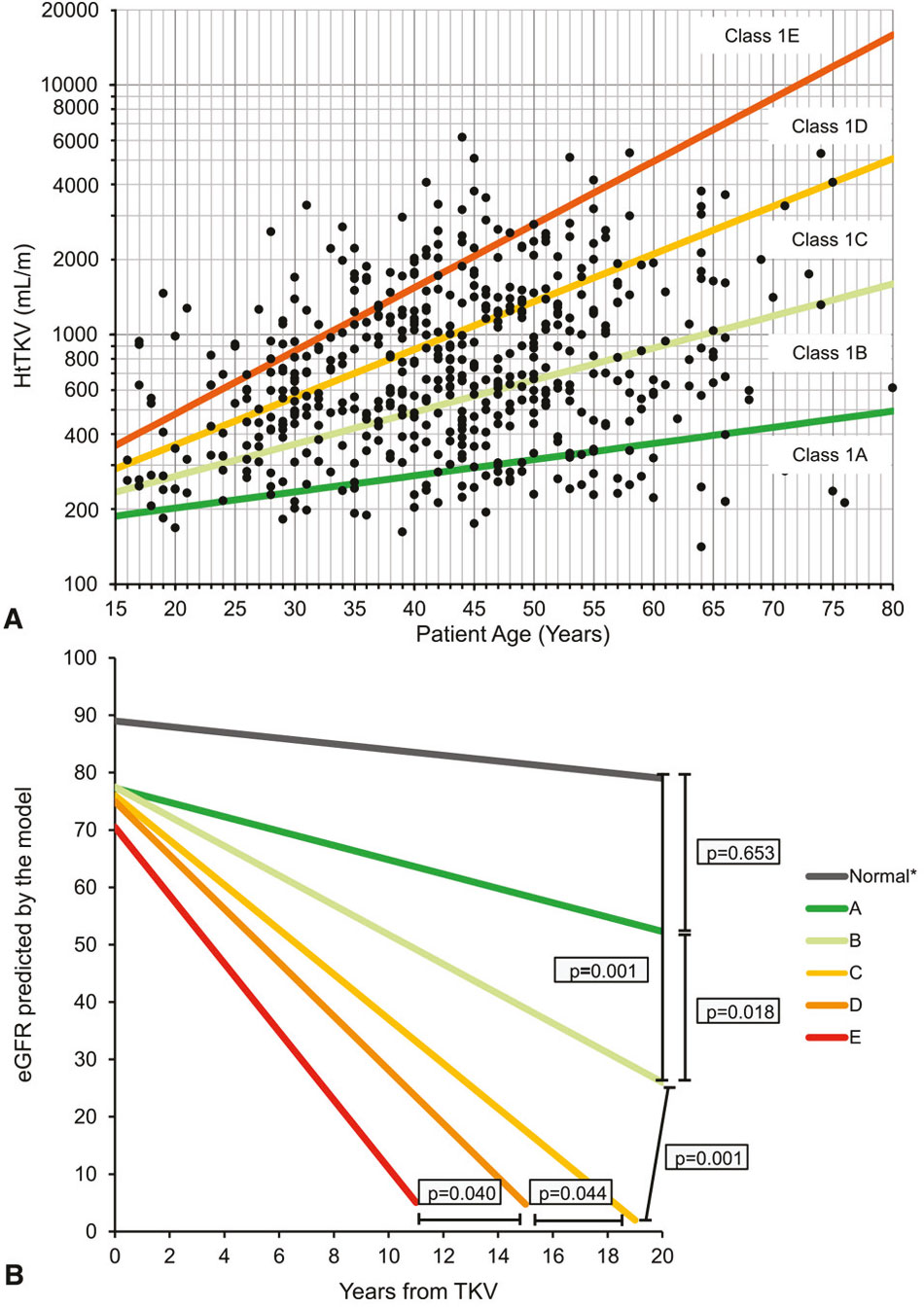
Figure 2. A, Subclassification of patients with class 1 autosomal dominant polycystic kidney disease at baseline based on htTKV and age at baseline. B, Predicted change in eGFR over time in class 1 patients (slopes shown are those for men).
Source. Republished from Irazabal et al29 with permission of the American Society of Nephrology; permission conveyed through Copyright Clearance Center, Inc.
Note. htTKV = height-adjusted total kidney volume; eGFR = estimated glomerular filtration rate; TKV = total kidney volume.