Preoperative Mapping for Upper Abdominal and Presternal Catheters
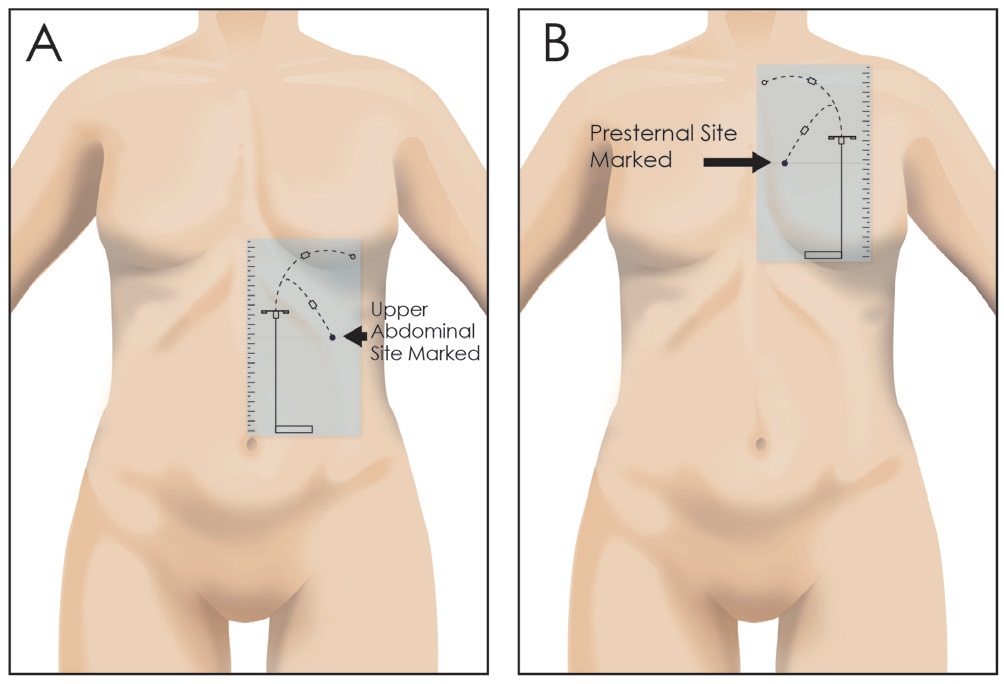
Figure 4. With the patient sitting, stencils can be used to select a suitable upper abdominal or presternal exit-site. Only the swan neck bend pattern of the stencil is used for marking because all commercially available extended catheters are equipped with preformed arc bends. Figure 4A. The preformed arc bend is directed laterally for upper abdominal catheters. Figure 4B. The preformed arc bend is directed medially for presternal catheters.
Stencils are exceedingly helpful in determining optimal upper abdominal and presternal exit-site locations. Mapping for an upper abdominal exit-site begins with the patient in a sitting position. The stencil plate possessing cutouts for the secondary incision, tunnel configuration, and exit-site is positioned over the patient’s upper abdomen (Figure 4A). Align the medial border of the stencil with the midline of the abdomen. Adjust the stencil cranially or caudally until the exit-site cutout is in a position that is easily visible to the patient, does not conflict with belt line or bra line, is free of skin creases or blind side of skin folds, and does not fall on the apex of a bulging or floppy skin fold. Confirm that cutouts for the subcutaneous arcuate tunnel do not conflict with the costal margin. After achieving a suitable location, mark the skin at the exit-site cutout. If a suitable exit-site cannot be obtained, proceed to assessment for a presternal exit-site location.
Mapping for a presternal catheter exit-site is performed with the patient in a sitting position. Female patients should wear their normal bra in order to note the point of rise of the breast mound. The stencil plate, possessing cutouts for the secondary incision, tunnel configuration and exit-site, is positioned over the patient’s upper chest (Figure 4B). Align the medial border of the stencil with the midline of the chest. Adjust the stencil cranially or caudally until the exit-site cutout is in a position that is not in the open collar area, does not conflict with a possible future midline sternotomy, is free of the fleshy or bulging part of the breast, and does not conflict with the bra line. Confirm that cutouts for the subcutaneous arcuate tunnel do not clash with the clavicle. After achieving a suitable location, mark the skin at the exit-site cutout.
After a satisfactory upper abdominal or presternal exit-site has been marked, the patient assumes a recumbent position. Female patients should remove the bra at this point to duplicate the conditions present during the catheter implantation procedure. Measurements are made, recording the horizontal distance from the marked exit-site to the abdominal or chest midline and the vertical distance from the point of intersection of the horizontal line with the midline to a landmark such as the umbilicus for upper abdominal catheters or the jugular (suprasternal) notch for presternal catheters. Distinctive moles or scars also can be used as landmarks to locate the exit-site. Measure and record the distance from the selected exit-site to these distinguishing marks.