KEY ACTIVITIES
Prepare patient:
- Administer antistaphylococcal antibiotic preoperatively5, 9
-
- First-generation cephalosporin 1000 mg intravenously, 1 to 3 hours preoperatively
OR
-
- Vancomycin 1000 mg intravenously, administered approximately 12 hours preoperatively10*
- A prospective randomized trial determined that vancomycin was superior to cephalosporin or no treatment in reducing post-operative peritonitis10*
- If vancomycin is used, weigh potential benefits versus risk of resistant organisms**
- Perform surgical skin prep (use electric clipper to avoid skin nicks)3
Prepare catheter:
- Eliminate air from catheter cuffs prior to implantation by soaking and gently squeezing cuffs in saline solution5
* The half-life of vancomycin and cefazolin are different, possibly influencing the results of this study
** The epidemiology and resistance patterns contributing to peritonitis should be considered in determining the appropriate preoperative antibiotics
Insert catheter:
Catheter implantation approaches include laparoscopic, laparoscopic-assisted, open dissection, and percutaneous needle-guidewire with or without image guidance. The following general guidelines should be adhered to irrespective of implantation technique chosen:
- Preoperative determination of most appropriate catheter type, insertion site, and exit-site location
- Use of double cuff catheter preferred11
- Paramedian insertion through body of rectus muscle and sheath to provide optimal catheter immobilization and minimize risk of pericatheter leak and hernia (Figure 7)5
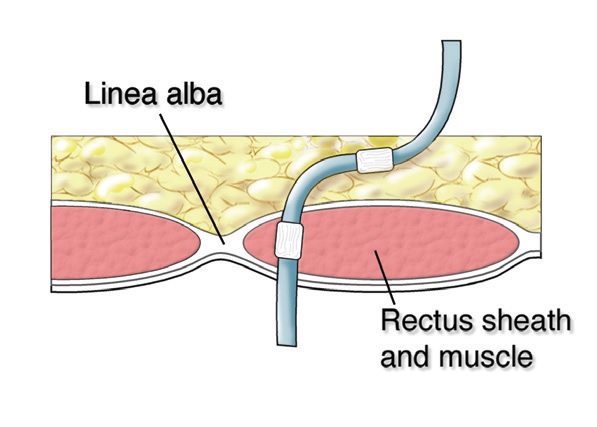
FIG. 7
Peritoneal dialysis catheter implanted through paramedian approach with deep cuff resting within the muscle.
- Position deep cuff within rectus muscle sheath5
- Implanting deep cuff superficial to rectus fascia can lead to formation of hernia or pseudohernia and late pericatheter leak (Figure 8)5
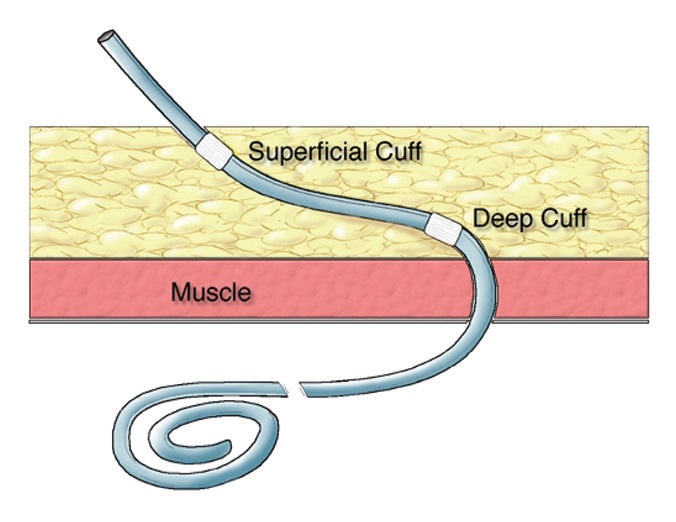
FIG. 8
(Top) Deep catheter cuff implanted external to the fascia. The mesothelium from the peritoneal surface reflects along the surface of the catheter to reach the deep cuff.
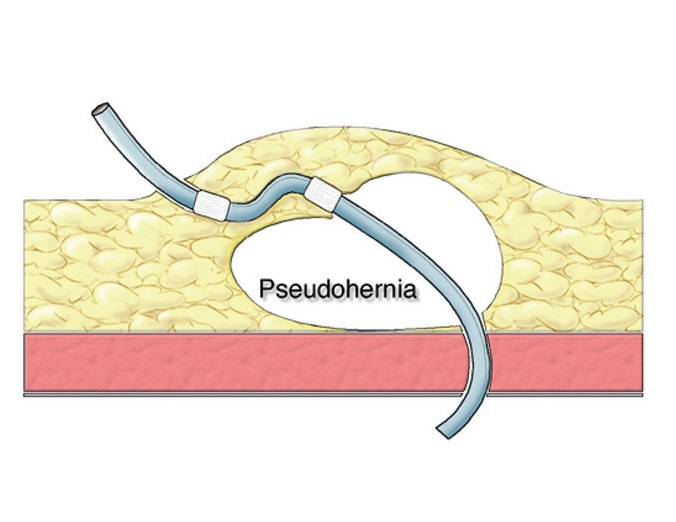
(Bottom) The extension of the peritoneal lining above the muscle layer creates the potential for a pseudohernia and pericatheter leak. If the abdominal wall is weak, the track may dilate and develop a true hernia.
Illustrations courtesy of John Crabtree, MD
- Catheter tip should have pelvic location5
- Place purse-string absorbable suture at level of peritoneum during open dissection or anterior rectus fascia with laparoscopic or percutaneous insertion to reduce risk of pericatheter leak5
- Catheters with straight intercuff segment should not be bent excessively in subcutaneous tissues to avoid creating shape memory resiliency forces that can lead to catheter tip migration and superficial cuff extrusion (Figures 9 and 10)3
- Subcutaneous tunneling instruments should not exceed diameter of dialysis catheter and should be capable of being advanced in direction from insertion site toward exit-site
- Create the smallest skin hole possible to provide for catheter exit-site5
- Position subcutaneous cuff 2 to 4 cm from exit-site5

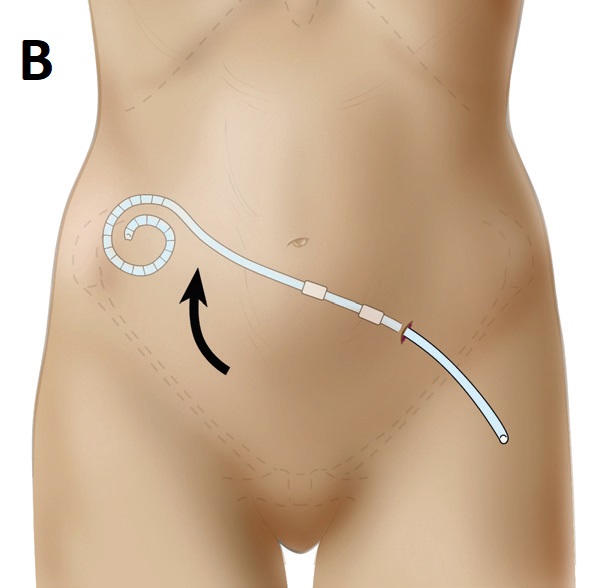
FIG. 9
(A) Straight catheter implanted into arcuate +configuration.
(B) Shape memory can cause catheter tip migration out of the pelvis.
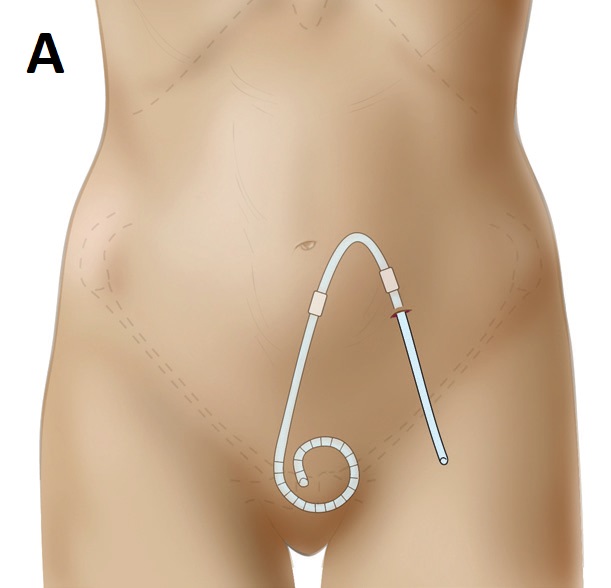
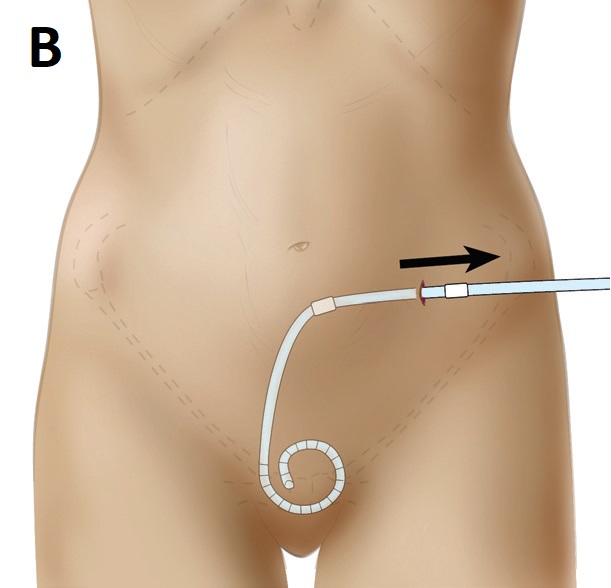
FIG. 10
(A) Straight catheter implanted into arcuate configuration.
(B) Shape memory can cause the superficial catheter cuff to extrude through the exit-site.
- Exit-site should face downward or lateral5
- Immobilize catheter with medical adhesive tincture (if available) and sterile adhesive strips2
- Do not utilize catheter anchoring sutures at the exit-site due to risk of infection5
- Perform adjunctive procedures to catheter implantation such as hernia repair, omentopexy, omentectomy, and adhesiolysis as needed
Verify function:
- Catheter patency and flow must be tested during surgical procedure prior to final closure. With the patient in reverse Trendelenburg position, a trial irrigation is performed by infusing a standard 1-liter bag of normal saline with heparin (1000 U per liter) and observe for unimpeded inflow and drainage by gravity. A residual volume of 250 to 300 mL is left in the abdomen to reduce the likelihood of intraperitoneal structures being siphoned up to catheter tip and side holes toward the end of the drainage phase
- Catheter position should be revised until satisfactory flow function is achieved before procedure end
- With non-laparoscopic implantation methods, it is advisable to check for catheter patency and flow prior to exteriorizing the catheter through the exit-site. This will prevent unnecessary tunnel track and exit-site trauma in the event that catheter repositioning is required.
Final catheter preparation:
- Insert catheter adapter
- Attach catheter cap or transfer set with cap (as per individual center policy)
- Make sure transfer set is in closed position
- Apply sterile gauze or other nonocclusive absorbent dressing and tape securely1, 12
- Tape catheter and transfer set securely to abdomen in several places
- Occlusive or semi-occlusive dressings may be used12